
There are a number of treatment options for both Jumper’s Knee and Runner’s Knee. All injuries need to be looked at individually and a number of factors need to be considered such as duration of symptoms, severity of symptoms, irritability of injury and other causative factors as outlined in Jumper’s Knee vs Runner’s Knee Part 1: What is the difference. Always speak to your physio before starting a rehabilitation plan.
Jumper’s Knee
Tendon’s mostly comprise of type-I collagen fibres which have viscous and elastic characteristics which can absorb large amounts of tensile load. Tendon’s are mostly avascular structures and need appropriate load to heal.
There are three stages in tendon healing: inflammation, proliferation, and remodelling.
Phase 1: Inflammation
This is the initial stage following in overload event and initiates the response to injury. This stage cause inflammatory cells (macrophages & fibroblasts) to enter the injury site. During this stage, neovascularisation occurs meaning there is new blood vessel production within the tendon.
Phase 2: Proliferation
These macrophages and fibroblasts then start to produce Type III collagen fibres and proteins to rebuild to cellular matrix of the injured tendon. However the cells are highly disorganised. This is when inappropriate loading of the affected tendon will cause a repetitive cycle between the inflammatory stage and the proliferation stage, further worsening the injury.
Phase 3: Remodelling
Appropriate loading is required to move into the remodelling phase. This is when scar tissue formation occurs and the cellular matrix of the tendon becomes much more organised. Vascularity of the tendon also decreases. Type III collagen converts to Type I collagen fibres to resemble the original tendon matrix.
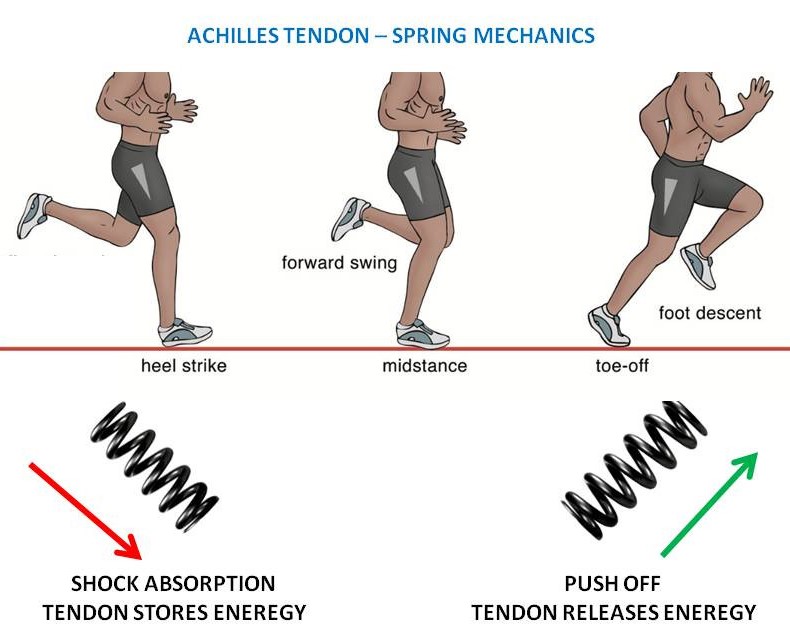
These changes to the tendon allow for greater energy storage capabilities and therefore able to produce greater force to propel you forward or upwards as you jump or run, just like a nice strong spring. The stronger the spring, the more energy it can absorb and release.
Below are a number of exercises that can help improve your pain and overall function of the knee.
Guidelines for Tendon Rehabilitation
Tendon’s need appropriate exercise to improve the overall performance of that tendon. However there are a number of exercise options depending on the severity of the injury. Pain is often a guide with exercise prescription for Jumper’s Knee. Similar to other tendon injuries, patient reported pain at 0-3/10 is the ideal zone and pain at 4-5/10 is acceptable. Any exercise or activity causing over 5/10 pain should be modified or stopped.
Isometric Wall Squat
Isometric exercises are the most basic and fundamental exercises in dealing with Jumper’s Knee. They are a good starting point to help alleviate pain. There are a number of different isometric options, however the wall squat is a good starting point.
Stand with your shoulders, back and hips against a wall and place your feet roughly 30-40cm away from the wall. Lower your body down towards the floor while your back and shoulders stay in contact with the wall. Once you are in a squat position, hold for 20-30 seconds before standing back up.
Eccentric Squat
This is an intermediate exercise in the rehab of Jumper’s Knee. This can also be added early in the rehab program if tolerated by pain.
Stand with your feet pointing downwards on a board with roughly a 45 degree angle. Lift your unaffected leg off the step and lower your body down slowly. Once you have reached a squat position, place your unaffected leg on the step to assist when standing back up. Repeat.
Bulgarian (Rear-Foot Elevated) Split Squat
This is a more advanced option for Jumper’s Knee rehabilitation once most of the acute pain has settled. You can increase the speed of the exercise and/or add weight to progress this exercise.
Place your unaffected leg on a step or bench behind you in a lunge position. Lower your body down towards the floor, placing most of your weight through your front leg and then stand back up. Repeat.
Once again, load is appropriate for tendon load. It is important to understand the limitations of your tendon and identify what load your knee can and can’t tolerate.
Runner’s Knee
Runner’s Knee often has many factors influencing the condition. One of which is running load. You will need to discuss training load with your physio or trainer to modify you exercise or running program to avoid injury and/or to prevent aggravating Runner’s Knee.
Hip Abduction on Wall
This is an exercise targeting gluteus medius and maximus. This is important to add strength to your lateral hip to help with the control of the knee in a single-leg stance position.
Lie on your side close to a wall and a slider/container lid between the wall and your heel. Apply pressure backwards onto the wall with your heel. Then slide your leg up and down the wall while maintaining that pressure on the wall. Make sure you keep your back straight.
Lunge with Medial Band
This exercise is adding extra gluteal activation into a functional exercise. The use of the band exaggerates the activation of the glute medius to avoid your knee from collapsing inwards when going into a lunge without the band.
Anchor a strong band against a wall. Stand in a lunge position with your affected leg forward and step into the band so that the band is against the outside of your leg. Lower your back leg down towards the ground. Make sure the knee of the front leg does not move inwards, ensuring your knee bends over your toes.
Single-leg Squat to Bench
In those suffering from Runner’s Knee, the knee will often drift inwards while performing squat based movements. This places more pressure on the patellofemoral joint. This exercise is targeting the stability of the knee and the hip to control the overall function of the knee joint.
Start by sitting on a bench or chair. Lift your unaffected leg off the floor. Stand up off the bench and then sit back down in a controlled manner. Repeat. Do not let your knee move inwards and do not let your body bend sideways.
Both of these injuries are very common with any running and jumping activity or sport. Monitoring and adapting training levels and activity loads are very important to managing both Jumper’s and Runner’s knee.
For more information please feel free to contact us, call us on 9280 2322 to chat to one of our physio’s, or book your appointment online.
