
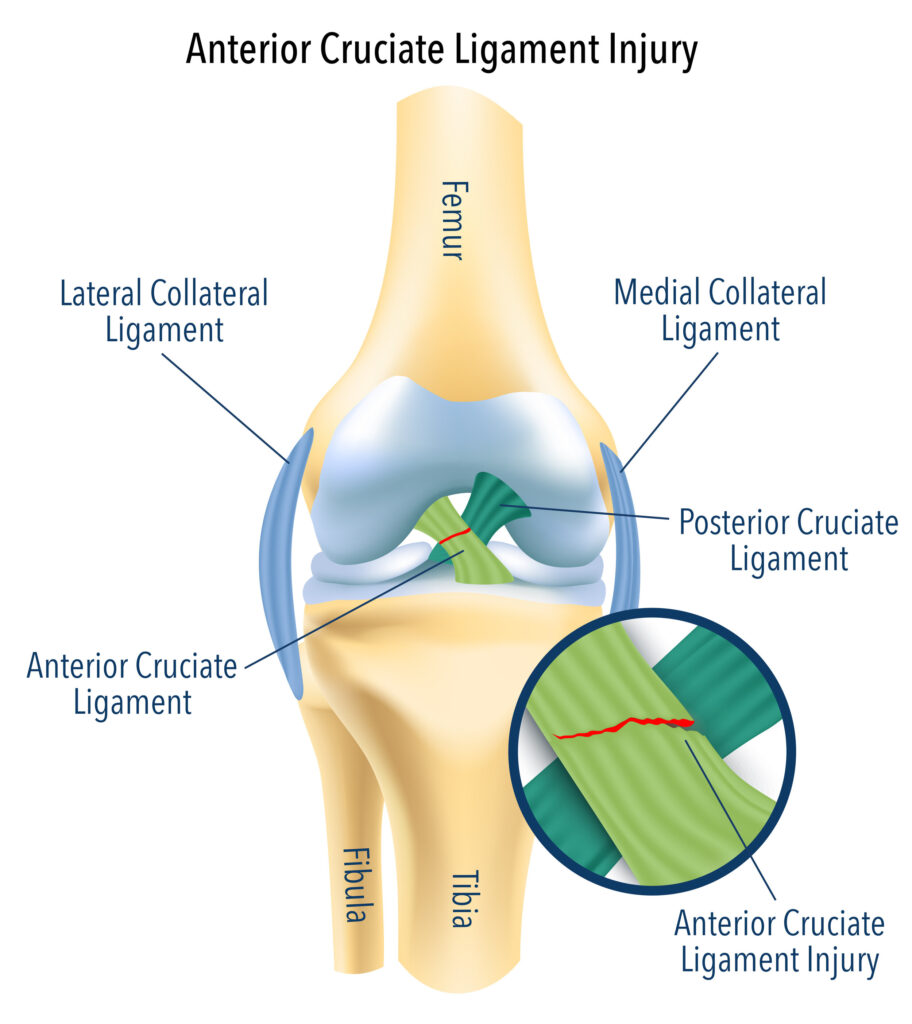
The ACL (Anterior Cruciate Ligament) makes up part of the internal structure of the tibiofemoral joint and is responsible for the overall stability of the knee joint. It is a dense bundle of connective tissue and is situated on the posterior aspect of the lateral femoral condyle and attaches to the anterior portion of the tibia.
The main role of the ACL is to limit the anterior translation of the tibia on the femur. In other words, it stops the tibia (shin) from moving forward in relation to the femur (thigh). It also important to prevent excessive rotation of the tibia on the femur.
ACL ruptures make up as high as 30% of all knee injuries in sport, particularly in sports which require change of direction and pivoting such as soccer, AFL, Rugby, Basketball and Netball. 70% of all ACL injuries occur without contact from landing poorly from a jump and sidestepping an opponent.
The reason why the ACL is talk about so much is the lengthy recovery. ACL injuries take anyway from 6 to 18 months to return to full function and return to sport. It also has a dramatic affect on long-term sport participation, overall knee health and function.
Today we are discussing the advantages and disadvantages of ACL reconstructions (ACLR) versus non-operative management of ACL injuries.
Surgical Intervention
ACL reconstructions have been the treatment of choice for ACL injuries for over the past 30 years. More recently, the amount of ACLR’s has increased significantly due to better imaging with MRI’s and the increase of people engaged in sport.
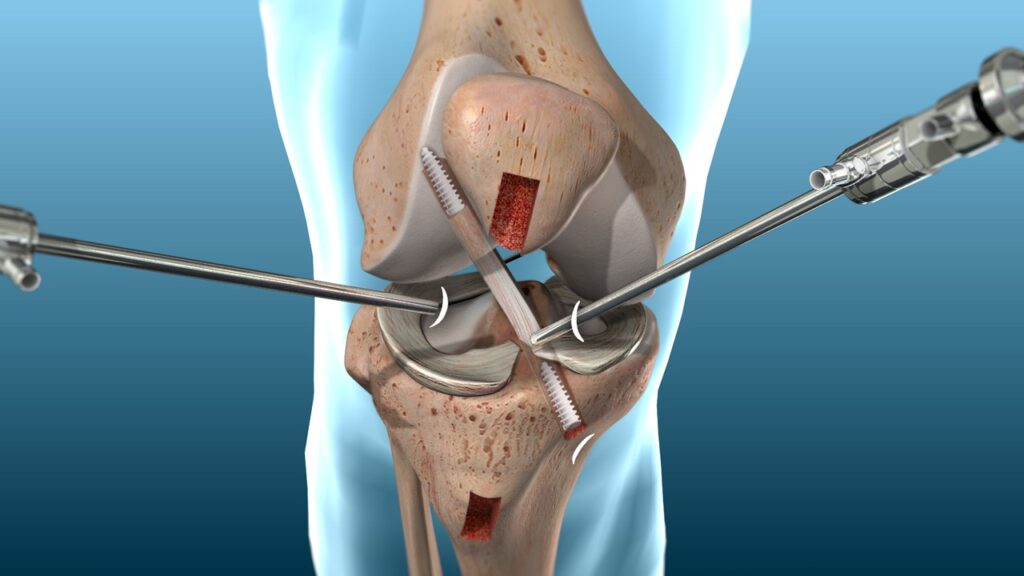
Surgical intervention involves arthroscopically removing the torn ACL and inserting a graft (connective tissue) where the ACL used to be. The grafts usually come from the hamstring tendon, patella tendon or quadricep tendon as seen below. The graft options will be determined by surgeon recommendations, patient preference and some individual factors such as age, type of sport you are returning to and previous knee injuries.
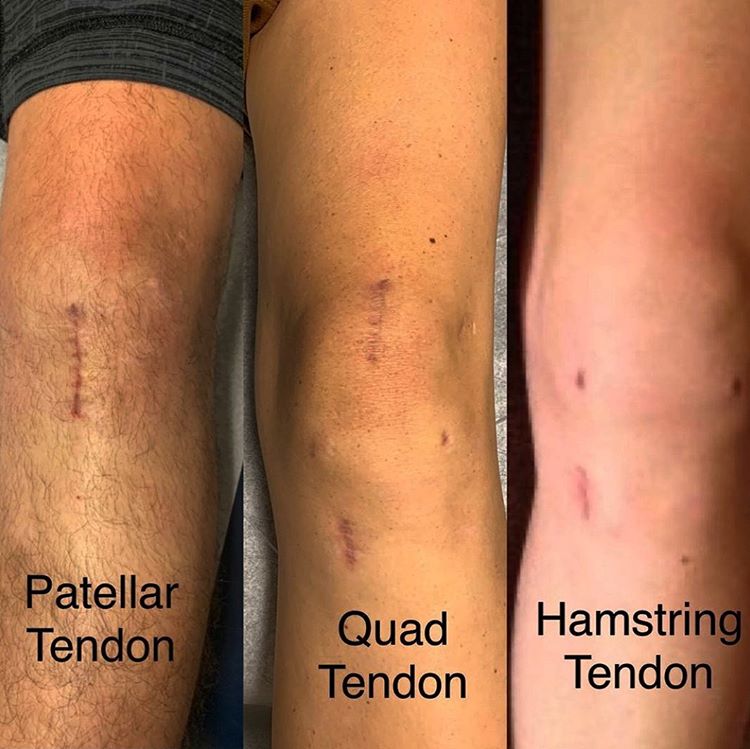
Hamstring Tendon
The hamstring tendon graft is done by stripping one or two of the hamstring tendons, usually the semitendinosus and/or semimembranosus. These two tendons are then intertwined the make up the hamstring graft. It is vital that the hamstring is also rehabilitated appropriately following the surgery to avoid any long-term hamstring issues.
Patellar Tendon
The middle portion of the patellar tendon is stripped to make up the graft. The patellar tendon is a very strong and thick tendon which provides a strong graft option. This option has an impact on strengthening the quadricep, particularly during the earlier stages of rehabilitation.
Quadricep Tendon
This is a newly trending graft option due to the improved graft technique options and fixation technology available. The benefit of using the quadricep tendon is the graft size and thickness is more reliable as well as being stronger compared to the hamstring. It is a new technique so there is limited research around the long term implementation of this graft.
There are also two main types of graft options;
Autograft
Tendon graft taken from one point to another of the same individual. This is the most common type of graft as most people prefer taking grafts from their own tissue and is less costly.
Allograft
Tendon graft from one individual to another. This method is often implemented when someone has had a number of ACL reconstructions in the past and have already taken a number of autografts.
Advantages of Surgical Intervention
Greater Knee Stability
The aim of an ACL reconstruction is to improve the overall stability of the knee joint by replacing the ruptured ACL with a graft to reduce the amount of anterior-posterior translation and rotation of the tibia on the femur. Without this, the knee will undergo more anterior-posterior translation leading to greater meniscus and cartilage trauma long-term. This statement is currently being argued against in some of the literature as there are only a few studies that actually validate this.
Return to sport
There are a large proportion of people that sustain ACL injuries in conjunction with meniscus, cartilage or other ligament injuries. In these circumstances, surgical intervention has been shown to be the more effective management strategy compared to non-operative management regarding returning to sport and returning to the same level of sport. For those that have self-selected the non-operative approach, only 20-40% of patients return to sport within 12 months and/or return to previous levels of activity.
Returning to sport is one of the most important influences for those who sustain ACL ruptures. For this reason having the ACLR is the more viable option, in some circumstances. At the moment it is also common practice to have the ACLR compared to not. There is lots of research surrounding ACL reconstruction’s and has been a proven option.
Disadvantages of Surgical Intervention
Cost
The average surgical cost of an ACL reconstruction is $8,364. This is not taking into account the costs involved in the lengthy 9-12 month rehabilitation required. In saying that, conservative management would also need a length rehabilitation which also incurs the same rehabilitation cost as return to sport usually occurs on average at the 12 months mark.
Barriers
As mentioned above, cost is heavily involved in ACLR recovery. This includes surgical and rehabilitation costs. Financial circumstances are one of the barriers to completing rehabilitation, along with adherence to rehab, work, family and other lifestyle barriers. Research has shown those that have limited obstacles to rehabilitation have better overall satisfaction with rehab, are more likely to return to sport by 12 months and return to the same level of activity.
Post-operative Symptoms
Pain, disability and reduced function are three main issues that occur immediately following an ACL reconstruction. There are significant amounts of swelling which cause pain and restriction of movement. Similarly, the pain of the operation itself will significantly impact the range of motion of the knee and function particularly in the few weeks post op. In some circumstances, walking braces and crutches are needed for the first 1-2 weeks. Despite swelling and pain occurring immediately after rupturing the ACL, this settles down within 1-2 weeks and the knee feels reasonably fine with day-to-day activities.


Long-term Knee Health
There are many studies looking at long-term knee function and health when comparing surgical versus non-surgical intervention. As non-operative management improves, the research indicates there is no long term difference between the two treatment options. This is regarding the development of knee osteoarthritis and/or development of meniscus pathologies at 5 to 15 years post injury. Follow-up studies throughout the literature and have all found similar results. Surgery can not guarantee better long-term knee health.
Non-operative Management
Non-operative management has become more common over the last 10 years. It involves rigorous rehabilitation to get the knee to functioning in a stable and controlled manner through all tasks including pivoting, landing and sudden changes of direction. More and more research is being conducted on non-operative management compared to operative management. There will be more to come and advocacy for non-operative management may change over the next 5-10 years.
Advantages of Non-operative Management
Return to Sport
Most people return to sport 9-18 months after undergoing an ACLR. However, evidence has suggested that returning to sport can occur within the same timeframe regardless of what treatment option you take. Most research allowed clients to choose whether they want to operate or not which has skewed the results to favor operative management. However, more recently, strict selection criteria for non-operative management is showing much more favourable outcomes. Up to 79% of people who were selected for non-operative management return to pre-injury activity levels with no episodes of instability.
Knee Stability
New research has indicated the use of a controlled motion brace within 4 weeks post ACL injury greatly improved the long-term stability of the knee joint alongside a structured rehabilitation program. Similarly, starting a non-operative program within two weeks post ACL rupture significantly improved the stability of the knee joint long-term. This contradicted the earlier suggestion that surgical intervention is what provided structural stability of the knee joint.
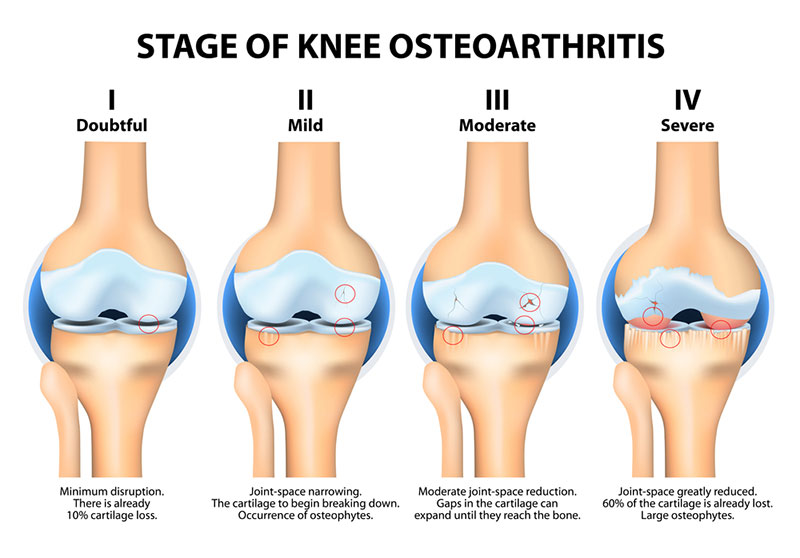
Risk of Osteoarthritis
Unfortunately knee osteoarthritis (OA) is more likely to occur in those that sustain ACL injuries. However, research has indicated that the likelihood of developing knee OA following an ACL injury is higher regardless of the treatment approach taken. The likelihood of developing knee OA are as follows:
- 4.2x greater risk for isolated ACL injury
- 6.3x greater risk for isolated meniscus injury
- 6.4x greater risk for combined ACL & meniscus injury
This indicates that long-term knee health is more dependent on the influences of the meniscus rather than the just ACL itself. There are a number of studies that have shown that OA development is present at 10-15 year follow-ups regardless of what management strategy is implemented. The reason this is an advantage for non-surgical management is because you may be able to have the same outcomes as someone that undergo surgery. It was previously thought that not having the ACLR will lead to OA development, however this has been proven to be wrong.
Cost
As mentioned above, non-operative management reduces the overall cost of ACL management. It is vital that rehabilitation is performed appropriately and adhered to, to reduce the ongoing complications involved with the knee joint. For this reason, there is still a cost involved is attending physiotherapy consults.
Disadvantages of Non-operative Management
Further Intervention
A number of studies have indicated that patients who opt for non-operative management following an ACL rupture undergo further surgery long-term. These surgeries include ultimately having the ACL reconstructed and/or meniscus surgeries. Some studies have shown as high as 80% of patients who go through non-operative management require surgery to remove part of the meniscus. This is thought to be due to the gradual degeneration of the meniscus due to the instability of the knee joint without an ACL. As mentioned above, careful selection criteria has significantly reduced the need for further intervention. This is something to keep a close eye so watch this space.
Long-term Symptoms
Instances of instability in the knee and some degree of pain can be expected when opting for non-operative management of the ACL. This may affect knee function and quality of life. As there is no physical structure preventing anterior translation of the knee, the sensation of instability is common. In saying so, having the ACLR does not mitigate these symptoms.
Adherence to Rehabilitation
Adherence to non-operative management is integral for it’s success. It only takes two to three months post injury for the knee to feel 100% with little to no pain or swelling. It is at this point that non-operative management drops off and patients do not continue with important stages of rehabilitation needed for returning to sport. As mentioned above only 20-40% of self-selected clients who undergo non-operative management return to pre-injury levels of sport. Being committed to non-operative management is key!
So which option is best?
This is a very tricky questions. At the moment, surgery is still the preferred option for patients that have co-existing injuries associated with the ACL, i.e. meniscus tears and/or cartilage damage. There is a lot of research around operative ACL management and most physio’s should have a good understanding of how to rehabilitate ACLR’s and get patients back to sport.
On the other hand, those that fit a particular criteria may benefit from not having the ACL reconstruction. Non-operative management is relatively new compared to surgical intervention. More research is needed. At this stage, there is no difference between those opting for ACLR’s or non-operative regarding long-term knee health. In that regard, patients that have isolated ACL injuries may benefit from non-operative management.
All factors need to be considered. If you are 15-30 years of age and returning to change of direction and pivoting sports, you may be more inclined to have surgical intervention. If you are only returning to straight line running then surgical intervention may not be needed. Talk to your physio and specialist to determine what the best option is for you. Your goals and expectations need to be also considered.
References
Kessler, M.A., Behrend, H., Henz, S. et al. Function, osteoarthritis and activity after ACL-rupture: 11 years follow-up results of conservative versus reconstructive treatment. Knee Surg Sports Traumatol Arthr 16, 442–448 (2008).
Fitzgerald, G., Axe, M. & Snyder-Mackler, L. A decision-making scheme for returning patients to high-level activity with nonoperative treatment after anterior cruciate ligament rupture. Knee Surgery 8, 76–82 (2000).
Park, YG., Ha, CW., Park, YB. et al. Is it worth to perform initial non-operative treatment for patients with acute ACL injury?: a prospective cohort prognostic study. Knee Surg & Relat Res 33, 11 (2021).
Cohen, M., Amaro, J. T., Ejnisman, B. et al. Anterior cruciate ligament reconstruction after 10 to 15 years: association between meniscectomy and osteoarthrosis. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 23(6), 629-634 (2007).
Poulsen E, Goncalves GH, Bricca A, et al. Knee osteoarthritis risk is increased 4-6 fold after knee injury – a systematic review and meta-analysis. British Journal of Sports Medicine, 53:1454-1463 (2019).
